
FOOSH Injury: Why it can cause wrist pain
What it is and why it need to be assessed properly
“FOOSH” is not just the sound that a skydiver makes while hurtling through the air. It is also commonly used medical acronym which stands for Falling On OutStretched Hand. When we fall, one of our neurological responses is to extend and outstretch our arm. This is a fairly hardwired response in our neurological systems designed to protect more important structures like our brains and viscera from hitting the ground during a fall. Unfortunately this also puts our extremities, especially our hands, wrists and shoulders at risk. If we look at this from a natural selection perspective, it makes a lot of sense to sacrifice our hands and wrists in order to protect our heads and necks. But injury to the upper extremity should not be overlooked, especially certain pathologies that can occur to the wrist as a result of FOOSH.
The wrist is one of the most commonly injured areas as a result of a FOOSH injury. Unlike its lower extremity cousin; the ankle, the wrist is not designed to withstand extremely large amounts of force. The wrist itself is composed of the end of the arm bones; the radius (thumb side) and ulna (pinky side). These connect to 8 irregularly shaped pebble like bones that form 2 rows in our wrist. These bones are connected by numerous ligaments and connective tissues, as well as have various blood supplies and innervations.
The most commonly injured of these irregularly shaped bones (carpals) is the scaphoid bone. It sits underneath the thumb in the row of metacarpals closest to the body. Typically when individuals hurt this bone they have pain in the area known as the anatomical snuffbox (pictured below) of the wrist. They will also have swelling and decreased range of motion in the wrist as well. The athletes that commonly get injured here are ones that are likely to fall onto outstretched hands like snowboarders, gymnasts, and skiers.

Circled is the anatomical snuffbox of the wrist
While injuries and fractures to the scaphoid are common, there are some nefarious aspects to a fracture in this bone that warrant investigation and proper assessment. We stated earlier that there are various blood supplies to the bones in the wrist. The tricky part of the plumbing in the wrist is that in order for blood to be pumped into the bones next to the scaphoid, the artery has to run through a ligament that is connected directly to the scaphoid itself (the scapholunate ligament for you anatomy nerds out there. Fractures of the scaphoid can also damage this ligament, which will also damage the blood supply to the bones next to the scaphoid, namely the lunate. Unfortunately this sets in motion a process called osteonecrosis, in which the lunate begins to deteriorate and die because of the loss of blood supply. This presents a pretty nasty scenario in the wrist which typically has to be managed surgically with either removal of the bone which is decayed or removal of the entire proximal row.
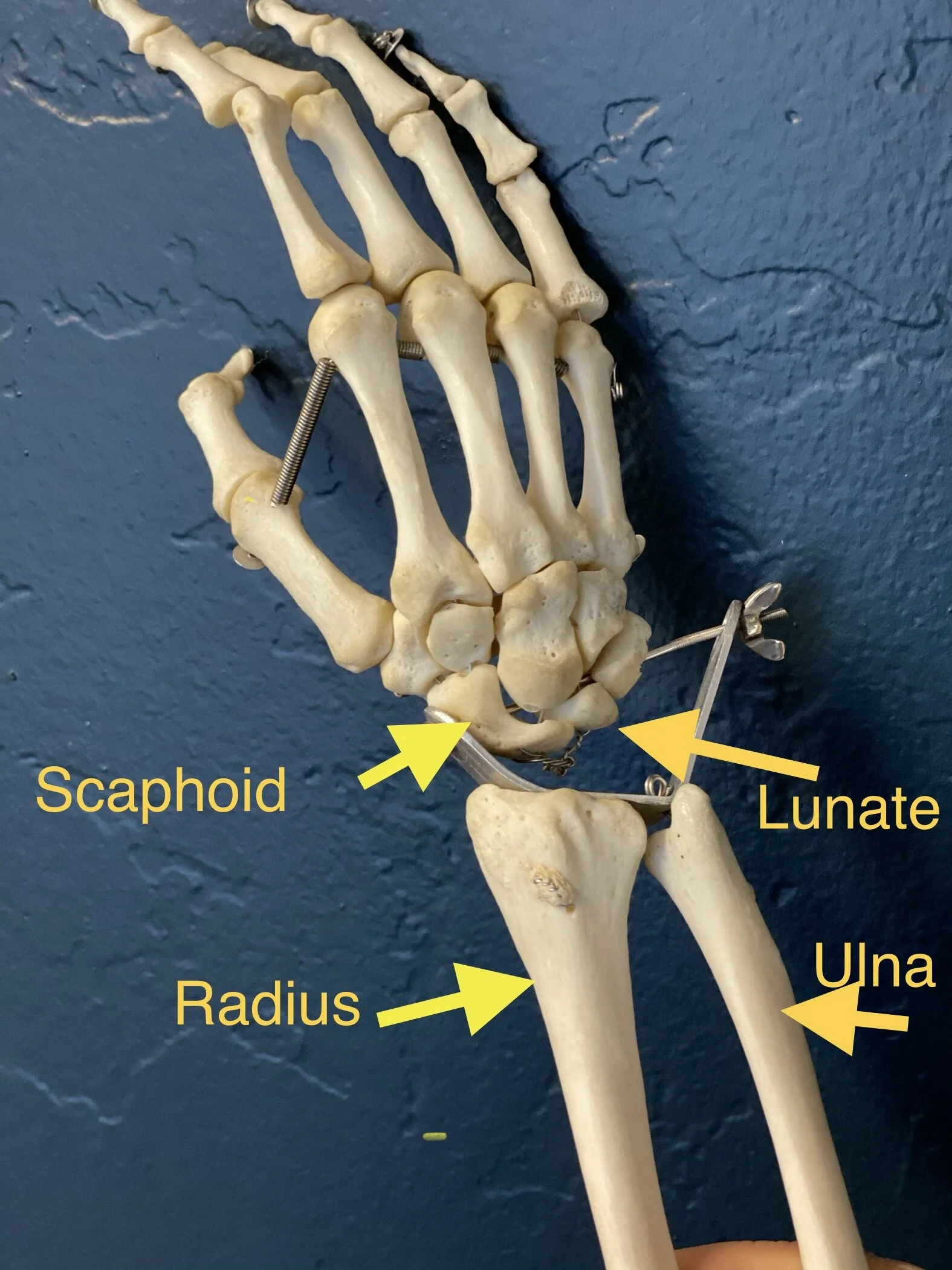
Labelled are the scaphoid, lunate, radius and ulna of the wrist.
Needless to say it is crucial that fractures to the scaphoid be properly assessed and managed in order to not place the adjacent carpals in harm's way. The first order of business after a traumatic fall or injury to the wrist is to get a specific x-ray series to take a look at the scaphoid. We are lucky enough to have an x-ray unit in the office, with which we can take a great look at the scaphoid. While we have a very good digital and modern unit in the office, small fractures can still be missed on the initial x-rays, so if there is still a chance of a fracture, we will typically take another set of x-rays about a week later. In such small bones as those we are looking at in the wrist, the time between x-rays allows calcium to be taken up in the areas of the fracture line, which will make them more prominent and easier to see. We will also be able to potentially see if there is damage to the bone next to the scaphoid on the second x-ray. If there is then we will promptly refer you out to receive an orthopedic consult and likely further imaging. In this case there is still time to receive the proper surgical care that will save the wrist in the long run. That is why it is so important to take the follow-up x-rays if a fracture isn’t seen initially, but is still suspected.
All of the nasty stuff aside, We can also get injuries in this type of fall that are not fractures to these bones. There are tons of tendons, muscles, ligaments, and nerves that can become damaged in a FOOSH incident. Many of these can be managed conservatively (not requiring surgery). Conservative management for wrist injuries may include various types of passive care such as needle therapy, class IV therapeutic laser, light manipulation, and strengthening exercises.
Needle therapy (acupuncture and dry needling) works by increasing blood flow to the damaged tissues, as well as increasing range of motion in the wrist, both of which will make our strengthening and rehab exercises more effective. Manipulation can be used in the case that the wrist is lacking range of motion due to excessively tight ligaments and dense connective tissues. Manipulation will help in increasing the range of motion, as well as decreasing pain in the wrist. Strengthening and range of motion (ROM) exercises are the real key to recovering from a wrist injury. It is really not too wrong to say that all of the passive therapies really just help us get to the strengthening exercises faster, and more effectively.